
Buprenorphine half-life is defined as the time it takes for the body to eliminate half of the drug from the bloodstream, and it ranges from 20 to 73 hours depending on the formulation and individual patient factors. For sublingual tablets, the standard form used in Suboxone therapy, the average falls closer to 31–35 hours. For extended-release depot injections like SUBLOCADE, that window stretches to weeks. Understanding what is buprenorphine half life matters because it directly shapes dosing schedules, withdrawal timelines, and what you or your loved one can expect during treatment.
What affects the half-life of buprenorphine?
Several factors determine how long buprenorphine stays active in the body. The two biggest are the formulation you take and the health of your liver.
Formulation type is the most immediate variable. Sublingual tablets and films dissolve under the tongue and enter the bloodstream gradually. Intravenous buprenorphine peaks faster and clears faster. Depot injections like SUBLOCADE release the drug slowly from a subcutaneous implant over weeks, producing a much longer apparent half-life.
Liver function is the second major driver. Buprenorphine is metabolized primarily by the liver through two enzymatic pathways: CYP3A4-mediated N-dealkylation and glucuronidation via UGT1A1 and UGT2B7. When those pathways are compromised, the drug clears more slowly. Specifically, moderate and severe hepatic impairment increases buprenorphine half-life compared to patients with normal liver function. That extended exposure raises the risk of drug accumulation over time.
Key factors that influence buprenorphine half-life include:
- Formulation: Sublingual, intravenous, and depot forms each produce distinct half-life profiles
- Liver health: Moderate to severe hepatic impairment slows clearance significantly
- Enzymatic activity: Genetic differences in CYP3A4 expression affect how fast the liver processes the drug
- Drug interactions: CYP3A4 inhibitors like ketoconazole or ritonavir can slow buprenorphine metabolism
- Body composition: Higher body fat can extend the drug’s distribution and apparent half-life
Notably, mild hepatic impairment does not cause clinically significant changes in buprenorphine pharmacokinetics. This distinction matters when your provider is deciding whether to adjust your dose.
Pro Tip: If you are taking any antifungal medications, HIV antiretrovirals, or antibiotics, tell your prescriber before starting buprenorphine. Several of these drugs inhibit CYP3A4 and can meaningfully extend how long buprenorphine stays in your system.

How do different buprenorphine formulations compare in half-life?
The difference between formulations is not subtle. It is the difference between a drug that clears in a day or two and one that remains detectable for over a year.
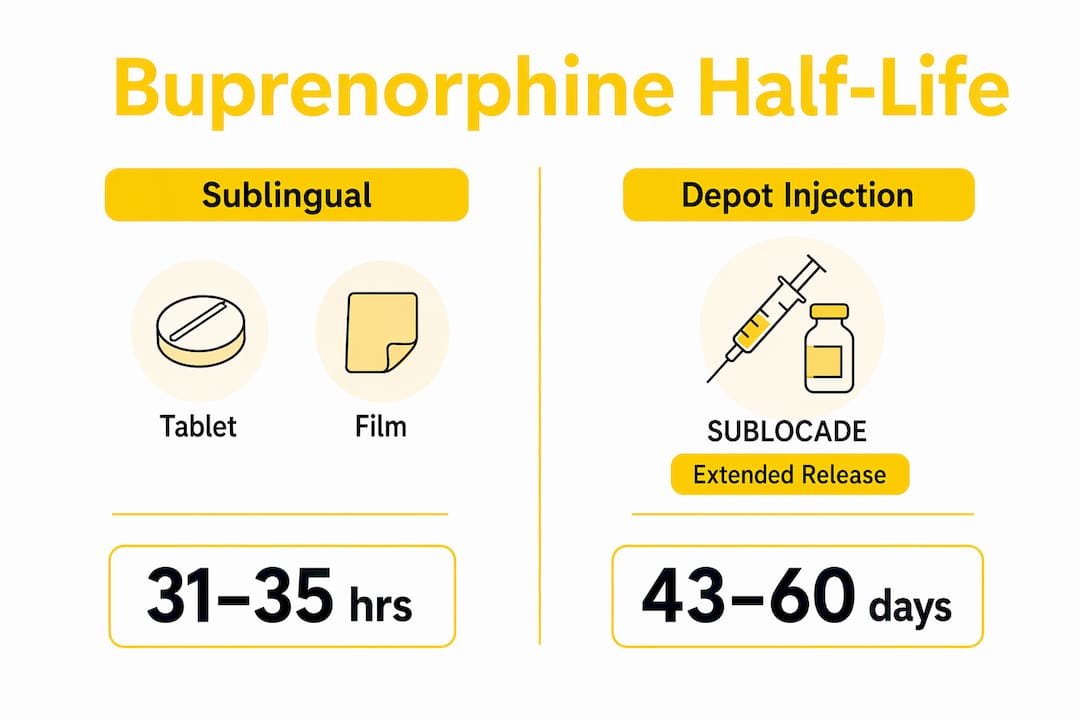
The mean half-life of sublingual buprenorphine tablets is approximately 31–35 hours. That means a single dose takes roughly three to five days to be mostly eliminated. This supports once-daily dosing for most patients, which is one reason sublingual Suboxone became the standard in Medication-Assisted Treatment.
SUBLOCADE, the extended-release subcutaneous depot injection, operates on a completely different timeline. Its apparent terminal plasma half-life is 43 to 60 days. That extended window results from the slow release of buprenorphine from the depot site rather than from the drug itself behaving differently once it reaches the bloodstream. The practical result is stable plasma levels with monthly dosing.
| Formulation | Typical Half-Life | Dosing Frequency | Detection Window |
|---|---|---|---|
| Sublingual tablet or film | 31–35 hours | Once daily | Days to weeks |
| Intravenous buprenorphine | 2–5 hours | Multiple times daily | Hours to days |
| SUBLOCADE depot injection | 43–60 days | Monthly | Up to 12+ months post-discontinuation |
This table shows why formulation choice is not just a convenience decision. It affects how quickly your provider can respond to side effects, how long the drug remains in your system after stopping, and how drug testing results should be interpreted. To understand more about how buprenorphine interacts with brain chemistry across these formulations, the brain mechanism guide from Mdmatt explains the pharmacology in plain language.
Pro Tip: Patients switching from sublingual Suboxone to SUBLOCADE should understand that plasma levels will not stabilize immediately. It takes several monthly injections to reach steady state, so early side effects or perceived underdosing are expected during that transition period.
What are the clinical implications of buprenorphine’s half-life?
The buprenorphine duration of action and its pharmacokinetic half-life are not the same thing. This distinction trips up patients and caregivers more than almost any other concept in opioid treatment.
Half-life tells you how long the drug stays in the blood. Clinical effect duration tells you how long it controls cravings and blocks withdrawal. For buprenorphine, the difference between these two measures is clinically significant. The drug’s partial agonist activity at the mu-opioid receptor and its high receptor binding affinity mean it can suppress withdrawal symptoms for 24 hours or longer even as plasma levels drop. That is why once-daily dosing works even though the half-life is only 31–35 hours.
For patients and caregivers, the most important clinical implications are:
- Withdrawal timing: After stopping sublingual buprenorphine, withdrawal symptoms typically begin 24–72 hours after the last dose. The long half-life delays onset compared to short-acting opioids like oxycodone.
- Drug testing: SUBLOCADE users should know that buprenorphine remains detectable in plasma and urine for 12 months or longer after discontinuation. A positive drug test after stopping treatment does not mean relapse.
- Dose adjustments in depot form: Because plasma concentration changes slowly after subcutaneous injection, dose adjustments do not rapidly alter blood levels. Providers cannot quickly correct over- or underdosing the way they can with sublingual forms.
- Liver impairment: Patients with moderate or severe hepatic impairment are contraindicated for depot buprenorphine. Prolonged half-life in these patients creates risk of dangerous drug accumulation.
Understanding your Suboxone dose variability in the context of these pharmacokinetic realities helps you have more productive conversations with your provider.
How is buprenorphine metabolized and cleared from the body?
Buprenorphine clearance follows a well-defined pathway through the liver and out through bile and urine. Here is how that process works step by step:
- Hepatic uptake: After absorption, buprenorphine travels to the liver, where it undergoes first-pass metabolism. This is why sublingual administration, which bypasses some first-pass metabolism, produces higher bioavailability than oral ingestion.
- CYP3A4-mediated N-dealkylation: The liver enzyme CYP3A4 converts buprenorphine into norbuprenorphine, its primary active metabolite. Norbuprenorphine has weaker opioid activity but still contributes to the drug’s overall effect profile.
- Glucuronidation: Both buprenorphine and norbuprenorphine are then processed by UGT1A1 and UGT2B7 enzymes into glucuronide conjugates. These conjugates are water-soluble and ready for excretion.
- Biliary and urinary excretion: Buprenorphine elimination occurs primarily through biliary excretion into the feces, with a smaller portion excreted through the kidneys in urine. This dual-route excretion means kidney disease alone rarely causes major accumulation.
The extensive hepatic metabolism via CYP3A4 and glucuronidation explains why liver health is so central to buprenorphine pharmacokinetics. Any condition or medication that disrupts these pathways will directly affect how long buprenorphine lasts in your body. For a broader look at how these metabolic factors connect to long-term treatment, the Mdmatt article on Suboxone long-term effects covers what patients should watch for over time.
Key takeaways
Buprenorphine half-life ranges from 31–35 hours for sublingual forms to 43–60 days for SUBLOCADE depot injections, and liver health is the single most important patient factor affecting clearance.
| Point | Details |
|---|---|
| Sublingual half-life | Sublingual buprenorphine averages 31–35 hours, supporting once-daily dosing for most patients. |
| Depot half-life | SUBLOCADE has a terminal half-life of 43–60 days due to slow subcutaneous release. |
| Liver function matters | Moderate to severe hepatic impairment extends half-life and raises accumulation risk. |
| Half-life vs. effect duration | Clinical effects last longer than plasma half-life suggests, due to high receptor binding affinity. |
| Post-discontinuation detection | SUBLOCADE remains detectable in plasma and urine for 12 months or more after stopping. |
What I have learned about half-life and patient expectations
One pattern I see repeatedly at Mdmatt is patients who feel confused or even alarmed when they learn how long buprenorphine stays in their system. They worry it means they are “still addicted” or that the drug is harming them. That concern is understandable, and it deserves a direct answer.
A long half-life is not a flaw in buprenorphine. It is one of the reasons the medication works so well. The extended presence in the body is what prevents the sharp peaks and valleys that drive cravings with shorter-acting opioids. Stability is the goal.
Where I think providers sometimes fall short is in explaining the difference between pharmacokinetic half-life and clinical effect duration before patients start treatment. When someone stops sublingual Suboxone and feels withdrawal symptoms 48 hours later, they are often surprised. They thought the drug would last longer because they heard it has a long half-life. That gap in understanding can shake confidence in the treatment.
For patients on SUBLOCADE, the counseling challenge is different. The drug’s presence for over a year after stopping is genuinely surprising to most people. I have seen patients panic over a positive drug test months after discontinuation, not realizing that result is expected and normal. Preparing patients for that reality upfront prevents a lot of unnecessary distress.
My honest recommendation: ask your provider to walk you through what your specific formulation’s half-life means for your withdrawal timeline, your drug testing, and your dosing schedule. You deserve that clarity before you start, not after something unexpected happens.
— Cory
Start your buprenorphine treatment with a team that explains everything
At Mdmatt, we believe you should never leave an appointment with unanswered questions about your medication. Our providers take the time to explain buprenorphine pharmacokinetics in plain language so you understand exactly what to expect from your treatment. Whether you are considering sublingual Suboxone or an extended-release option, our Suboxone treatment clinic in Maryland offers evidence-based, patient-centered care built around your specific needs. We also offer telehealth treatment services for patients who need flexible access to care. Reach out today and take the next step with a team that treats you with dignity.
FAQ
What is the half-life of buprenorphine sublingual tablets?
The mean elimination half-life of sublingual buprenorphine tablets is approximately 31–35 hours. This supports once-daily dosing in most Medication-Assisted Treatment programs.
How long does buprenorphine stay in your system after stopping?
For sublingual forms, buprenorphine clears within several days to a few weeks after stopping. For SUBLOCADE depot injections, plasma and urine levels can remain detectable for 12 months or longer after the last dose.
Does liver disease affect how long buprenorphine lasts?
Yes. Moderate and severe hepatic impairment increase buprenorphine half-life and slow clearance. Mild liver impairment does not cause clinically significant changes, but patients with serious liver disease require careful monitoring and may not be candidates for depot formulations.
Why does buprenorphine withdrawal start so long after the last dose?
Buprenorphine’s long half-life of 31–35 hours for sublingual forms delays the onset of withdrawal compared to short-acting opioids. Symptoms typically begin 24–72 hours after the last dose rather than within hours.
What enzymes break down buprenorphine in the body?
Buprenorphine is metabolized primarily by CYP3A4 in the liver, which converts it to norbuprenorphine. UGT1A1 and UGT2B7 then glucuronidate both compounds for excretion through bile and urine.

