
The opioid withdrawal timeline is defined as the sequence of symptom onset, peak intensity, and resolution that follows the last dose of an opioid. Clinically, this process is called opioid withdrawal syndrome, and understanding what is opioid withdrawal timeline means knowing that no two patients experience it identically. The timeline shifts significantly based on whether the opioid is short-acting or long-acting, how long you have been using it, and your overall health. Knowing what to expect before you begin reduces fear and helps you prepare for each phase with a clear head.
What are the typical phases of the opioid withdrawal timeline?
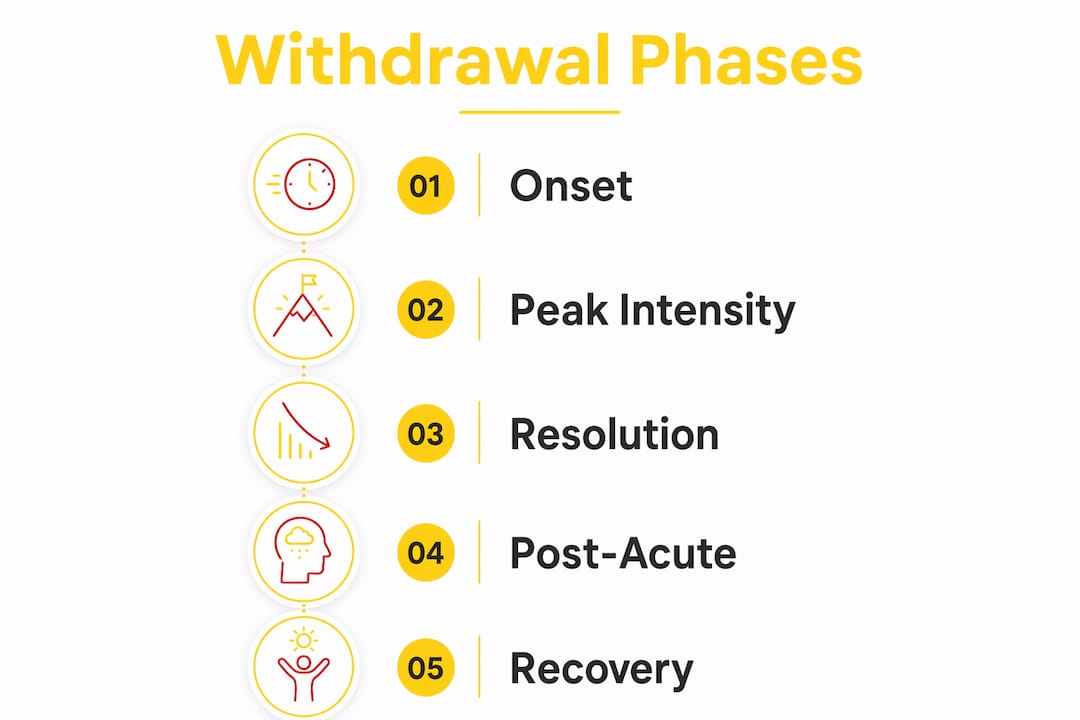
The opioid detox timeline moves through three distinct phases: onset, peak, and resolution. Each phase carries its own set of symptoms and its own level of intensity.
-
Onset. This is when your body first signals that opioids are leaving your system. Symptoms are usually mild at this stage. You may notice yawning, restlessness, runny nose, and mild anxiety. For short-acting opioids like heroin or oxycodone, onset begins within 6–12 hours after your last dose. That rapid arrival is a direct result of how quickly these drugs clear your bloodstream.
-
Peak. This is the hardest part. Symptoms reach their highest intensity and can include severe muscle aches, nausea, vomiting, sweating, and significant psychological distress. For short-acting opioids, the peak falls between 24 and 48 hours. For long-acting opioids, the peak arrives later but can be equally demanding.
-
Acute resolution. Symptoms begin to ease and become manageable. Physical discomfort fades first. Psychological symptoms like anxiety and insomnia tend to linger longer. For most short-acting opioids, acute withdrawal resolves within 5–7 days.
-
Post-acute phase. This phase is less discussed but equally real. Cravings and dysphoria can persist for weeks to months after acute symptoms clear. This extended neurochemical readjustment is one of the primary reasons relapse risk stays elevated long after the physical symptoms are gone.
Understanding these four phases gives you a map. You know the hardest stretch is temporary, and you know what comes after it.
How does the timeline differ between short-acting and long-acting opioids?
The type of opioid you have been using is the single biggest factor in shaping your withdrawal experience. Drug half-life determines how quickly your body registers the absence of the substance, which controls both when symptoms start and how long they last.
| Feature | Short-acting opioids | Long-acting opioids |
|---|---|---|
| Examples | Heroin, oxycodone, hydrocodone | Methadone, extended-release morphine |
| Onset | 6–12 hours after last dose | 12–48 hours after last dose |
| Peak intensity | 24–48 hours | Days 3–7 |
| Acute duration | 5–7 days | 10–20 days |
| Peak severity | High and rapid | Slower build, prolonged |
Short-acting opioids leave your system fast. That speed means symptoms arrive quickly and intensely, but they also clear faster. Long-acting opioids like methadone bind more deeply to receptors and release slowly. Methadone withdrawal onset is delayed by 12–48 hours, which can feel deceptive. You may feel fine the first day and then be caught off guard when symptoms arrive on day two or three and persist for up to 20 days.
Fentanyl deserves its own note. Despite being classified as short-acting, fentanyl’s retention in body fat creates an atypical withdrawal profile. Its lipophilicity means the drug continues releasing from fat stores after your last dose, making the withdrawal timeline more unpredictable and often more prolonged than other short-acting opioids. If fentanyl has been part of your opioid use, expect variability and plan for a longer acute phase.
Pro Tip: If you are transitioning from methadone or fentanyl to Suboxone (buprenorphine), timing is especially critical. Starting Suboxone too early can trigger precipitated withdrawal. Read the safe start guide from Mdmatt before your first dose.
What symptoms occur throughout the withdrawal process and how do they change?
Opioid withdrawal symptoms include yawning, sweating, nausea, anxiety, insomnia, gastrointestinal distress, and muscle aches. They do not all arrive at once. They build in layers, which is why understanding the stages of opioid withdrawal matters so much.
Early symptoms are flu-like and uncomfortable but manageable:
- Yawning and watery eyes
- Runny nose and goosebumps
- Mild anxiety and restlessness
- Low-grade muscle tension
As you move into the peak phase, symptoms intensify significantly:
- Severe muscle cramps and bone pain
- Nausea, vomiting, and diarrhea
- Profuse sweating and chills
- Elevated heart rate and blood pressure
- Insomnia and significant psychological distress
Autonomic symptoms like tachycardia and elevated blood pressure are worth taking seriously. They are rarely life-threatening in otherwise healthy adults, but they can become dangerous without monitoring. This is one of the clearest reasons medical supervision matters during the peak phase.
Pro Tip: Tracking your symptoms daily using a simple journal helps you and your care team see whether you are progressing normally or need additional support. Mdmatt uses structured clinical assessments to guide this process.
Post-acute withdrawal syndrome, sometimes called PAWS, is the phase most patients do not anticipate. Cravings, mood swings, and a general sense of emotional flatness can persist for weeks to months. This is not weakness. It is your brain’s neurochemistry recalibrating after a period of dependence.
How can knowing the timeline help you manage symptoms effectively?
Knowing the duration of opioid withdrawal gives you a concrete framework for planning. That framework reduces panic during the hardest days because you understand that the peak is temporary and that relief is measurable in days, not an indefinite stretch.
Several evidence-based strategies reduce symptom severity across the withdrawal timeline:
- Gradual tapering. The CDC recommends tapering at approximately 10% per month for long-term opioid patients. This rate allows your nervous system to adjust incrementally rather than facing an abrupt absence of the drug.
- Clinical Opioid Withdrawal Scale (COWS). The COWS assessment scores 11 observable signs to measure withdrawal severity. Clinicians use it to decide when to start medications and how to adjust dosing. You can ask your provider to walk you through your COWS score at each visit.
- Medication-Assisted Treatment (MAT). Suboxone (buprenorphine/naloxone) is one of the most effective tools for managing withdrawal symptoms and reducing cravings. It works by partially activating opioid receptors, which eases symptoms without producing a high. Understanding what precipitated withdrawal is before starting Suboxone protects you from a painful setback.
- Clonidine. This non-opioid medication targets autonomic symptoms like elevated heart rate and blood pressure. It does not address cravings but meaningfully reduces physical discomfort during the peak phase.
- Naloxone awareness. Less than 1% of naloxone-precipitated withdrawal cases require hospital admission. That statistic shows that naloxone is safe in appropriate clinical settings, but it also confirms that precipitated withdrawal is a real risk that requires professional guidance.
Medical supervision is not optional for patients with long-term or high-dose opioid use. The psychological distress during peak withdrawal carries real risks, including relapse and, in severe cases, suicidal ideation. A clinician who monitors your progress can intervene early if symptoms escalate beyond what home management can address.
Key Takeaways
The opioid withdrawal timeline is predictable by opioid type, and knowing each phase gives you the clearest possible path through it.
| Point | Details |
|---|---|
| Timeline varies by opioid type | Short-acting opioids resolve in 5–7 days; long-acting opioids can last 10–20 days. |
| Peak phase is the hardest stretch | Symptoms peak at 24–48 hours for short-acting opioids and days 3–7 for long-acting opioids. |
| Fentanyl is unpredictable | Fat retention makes fentanyl withdrawal longer and less predictable than other short-acting opioids. |
| Post-acute symptoms persist | Cravings and dysphoria can last weeks to months and require ongoing support beyond acute detox. |
| Medical supervision reduces risk | COWS assessments, tapering, and medications like Suboxone significantly reduce symptom severity and relapse risk. |
What I have learned from watching patients move through withdrawal
By Cory
The part that surprises most patients is not the physical pain. They expect that. What catches them off guard is the psychological weight of the post-acute phase, those weeks after the acute symptoms clear when they feel emotionally flat and wonder if they will ever feel normal again.
I have seen this pattern enough times to say it clearly: that flatness is not a sign that something went wrong. It is your brain doing the slow, unglamorous work of restoring its own chemistry. The neurophysiological adaptation that drives dependence took months or years to develop. It does not reverse in a week.
The other misconception I push back on constantly is the idea that withdrawal is a moral test. It is not. Opioid dependence is a neurophysiological condition. The flu-like symptoms, the anxiety, the insomnia are your nervous system responding to the absence of a substance it has reorganized itself around. That is biology, not character.
What I wish more patients knew before they started: the biggest danger during withdrawal is not the physical symptoms. The greatest risk is psychological distress leading to relapse or, in severe cases, self-harm. That is why I believe so strongly in medically supervised withdrawal over going it alone. Not because patients are incapable, but because no one should have to navigate that level of distress without support.
— Cory
Mdmatt supports you through every phase of withdrawal
Withdrawal is hard. It does not have to be something you face without a clear plan and a team behind you.
Mdmatt is a Maryland-based outpatient clinic specializing in Suboxone treatment and Medication-Assisted Treatment for opioid use disorder. The clinical team uses structured assessments, individualized tapering plans, and compassionate care to help patients move through each phase of withdrawal safely. Mdmatt also offers telehealth treatment services for patients who need flexible access to care. Whether you are in the early planning stage or already in the middle of withdrawal, reaching out to a medical provider is the most effective step you can take right now.
FAQ
How long does opioid withdrawal last?
The duration of opioid withdrawal depends on the opioid type. Short-acting opioids like heroin resolve within 5–7 days, while long-acting opioids like methadone can produce symptoms lasting 10–20 days.
When do opioid withdrawal symptoms start?
Short-acting opioid withdrawal begins within 6–12 hours of the last dose. Long-acting opioid withdrawal has a delayed onset of 12–48 hours, which can make the start feel deceptive.
What does peak withdrawal feel like?
Peak withdrawal typically involves severe muscle aches, nausea, vomiting, sweating, elevated heart rate, and significant anxiety. For short-acting opioids, this peak hits at 24–48 hours after the last dose.
Is fentanyl withdrawal different from other opioids?
Yes. Fentanyl is stored in body fat, which causes a more prolonged and unpredictable withdrawal timeline compared to other short-acting opioids. Patients should expect more variability and plan for a longer acute phase.
Can Suboxone help with opioid withdrawal symptoms?
Suboxone (buprenorphine/naloxone) is one of the most effective medications for managing withdrawal symptoms and reducing cravings. Timing the first dose correctly is critical to avoid precipitated withdrawal, which is why medical supervision is strongly recommended.

