The DEA waiver for buprenorphine, formally known as the X-waiver, is a federal authorization that once required clinicians to obtain special permission before prescribing buprenorphine to treat opioid use disorder (OUD). As of june 8, 2026, the DEA formally removed this requirement entirely. Any clinician holding a standard DEA Schedule III registration can now prescribe buprenorphine without special federal authorization. This change affects both healthcare providers navigating buprenorphine prescribing rules and patients seeking access to medication-assisted treatment (MAT) for opioid use disorder.
What is the DEA waiver for buprenorphine, and why did it exist?
The X-waiver was created under the Drug Addiction Treatment Act of 2000, commonly called DATA 2000. It required physicians, nurse practitioners, and physician assistants to complete specific training and register separately with the DEA before they could prescribe buprenorphine for OUD. The intent was to expand office-based treatment beyond methadone clinics while maintaining oversight. In practice, the waiver created a significant barrier. Clinicians who wanted to help patients with OUD had to jump through extra federal hoops that did not apply to any other Schedule III controlled substance.
The X-waiver requirement stood for more than two decades before federal policy caught up with public health need. The opioid crisis deepened, treatment gaps widened, and advocacy from medical organizations, public health experts, and patients made the case that the waiver was doing more harm than good by limiting the number of providers who could offer this life-saving medication.
How did the DEA waiver requirement get removed?
The removal did not happen overnight. It was the result of layered legislative action over several years:
- DATA 2000 (2000): Created the X-waiver system, requiring special DEA authorization for buprenorphine prescribing in office-based settings.
- SUPPORT Act (2018): Expanded eligibility for the X-waiver to nurse practitioners and physician assistants, and reduced some training burdens, but kept the waiver itself in place.
- Consolidated Appropriations Act (2022): Eliminated the X-waiver requirement entirely for most prescribers, though implementation rules were still pending.
- DEA Final Rule (june 2026): Implemented the 2022 Act’s provisions, formally ending the X-waiver and codifying new training requirements into standard DEA registration.
The driving force behind these changes was a clear public health priority: more providers needed to be able to offer buprenorphine treatment without bureaucratic delay. Advocacy from organizations like the American Medical Association, combined with mounting overdose data, pushed Congress and federal agencies to act. The goal was to treat OUD the same way medicine treats any other chronic condition, with standard clinical training and a regular prescription pad.
Who can prescribe buprenorphine now?
Any clinician with a valid DEA Schedule III registration can now prescribe buprenorphine for opioid use disorder. The removal of patient caps means there is no longer a federal limit on how many patients a provider can treat with buprenorphine at one time. Clinical judgment and state regulations now govern those decisions.
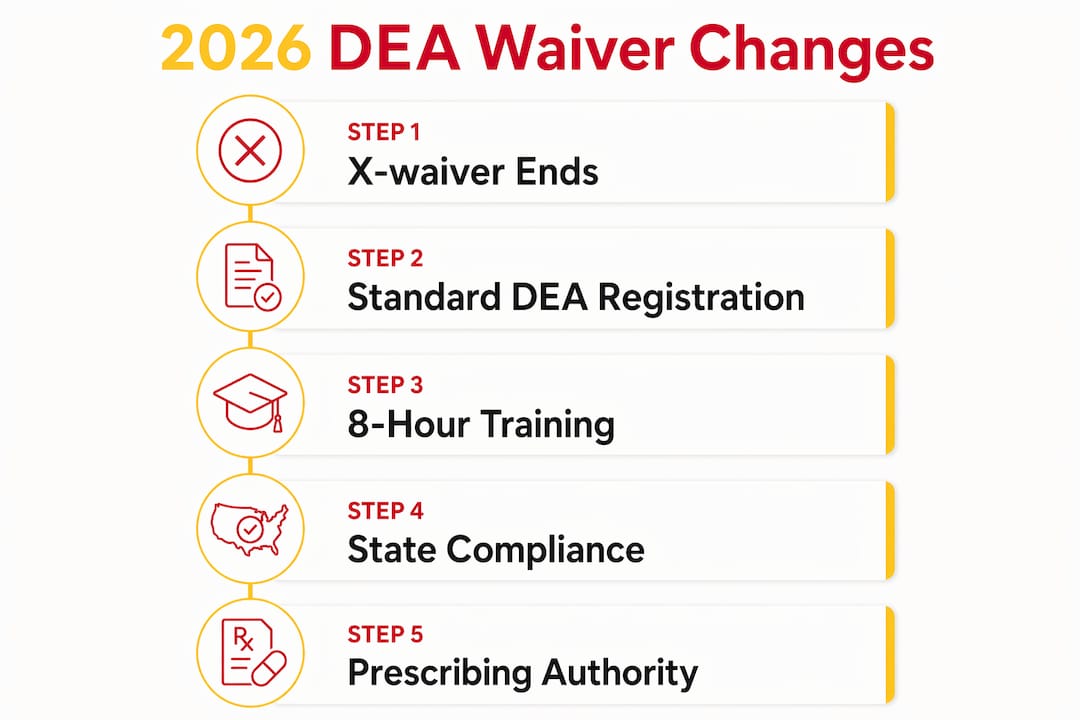
The updated federal requirements include:
- Standard DEA Schedule III registration: No separate X-waiver application or approval needed.
- One-time 8-hour training: Clinicians applying for new DEA registrations or renewing existing ones for controlled substances must complete 8 hours of training on substance use disorder treatment and management. This requirement applies to all controlled substance registrations submitted after june 27, 2023.
- No federal patient caps: The federal limit on the number of patients a provider can treat with buprenorphine has been eliminated.
- State law compliance: Providers must still follow state licensing rules, scope of practice laws, and any local regulations that apply to buprenorphine prescribing.
Pro Tip: The 8-hour training requirement can be completed in segments over time rather than in one continuous block. Clinicians can fulfill the requirement gradually alongside their other professional duties, which makes compliance far more manageable.
State laws remain a meaningful variable. Some states have additional licensing requirements or prescribing restrictions that go beyond federal rules. Providers should verify their state’s specific requirements before expanding their buprenorphine practice.
What operational changes do providers need to know?
The removal of the X-waiver changes more than just paperwork. It reshapes how buprenorphine treatment fits into clinical workflows, especially for primary care offices and emergency departments.
- Extended injectable MOUD window: The DEA’s final rule extended the administration window for long-acting injectable medications for opioid use disorder from 14 days to 45 days after receipt. This reduces the risk of wasted medication and gives providers more flexibility in scheduling.
- Inventory and destruction rules: Providers must track administration dates carefully. Unused long-acting injectable MOUD that exceed the 45-day window often require destruction under state law. Inventory management practices need to reflect this.
- Primary care and emergency integration: The elimination of special federal hurdles integrates buprenorphine prescribing into routine care settings, including primary care offices and emergency departments, where patients with OUD are frequently seen but historically undertreated.
- Telehealth prescribing: Providers can prescribe buprenorphine via telehealth, including audio-only platforms, under SAMHSA guidelines. This is especially relevant for reaching patients in rural or underserved areas.
| Change | Previous Rule | Current Rule (2026) |
|---|---|---|
| Prescribing authorization | X-waiver required | Standard DEA Schedule III registration |
| Federal patient cap | Yes, tiered limits | No federal cap |
| Injectable MOUD window | 14 days | 45 days |
| Training requirement | X-waiver specific | One-time 8-hour SUD training |
Pro Tip: If your practice is new to buprenorphine prescribing, start by auditing your state’s specific rules before seeing your first patient. Federal changes are now in place, but state compliance is where most providers encounter unexpected friction.
How does the waiver removal affect patients seeking treatment?
For patients, the removal of the X-waiver is one of the most meaningful policy changes in addiction medicine in years. The core impact is access. More providers can now offer buprenorphine treatment, which means shorter wait times and more options for where and how you receive care.
Key benefits for patients include:
- More providers available: Without the X-waiver barrier, primary care doctors, internists, and emergency physicians can now prescribe buprenorphine as part of routine care.
- Telehealth access: SAMHSA’s telehealth protocols allow buprenorphine to be prescribed via audio-only platforms, which is a significant gain for patients in rural areas or those with transportation barriers. Learn more about buprenorphine formulations and how telehealth prescribing works.
- Safer medication profile: Buprenorphine is a partial opioid agonist, which gives it a safer ceiling effect compared to full agonists like methadone. This profile makes it well-suited for telehealth initiation without the same level of in-person monitoring required for methadone.
- Comprehensive treatment plans: Buprenorphine works best as part of a broader treatment plan that includes counseling and support services. Access to individual counseling alongside medication significantly improves long-term outcomes.
Despite federal progress, state regulations and provider comfort levels still shape how accessible buprenorphine treatment is in practice. Not every provider will immediately begin prescribing, and not every state makes it equally easy. Patients may still need to seek out practices that specialize in addiction medicine or MAT.
Key Takeaways
The removal of the DEA X-waiver in 2026 is the single most significant regulatory change in buprenorphine prescribing since DATA 2000 created the waiver system more than two decades ago.
| Point | Details |
|---|---|
| X-waiver officially ended | As of june 8, 2026, standard DEA Schedule III registration is all that is required to prescribe buprenorphine. |
| No federal patient caps | Providers now use clinical judgment and state law to determine how many patients they treat. |
| 8-hour training required | All new or renewing DEA controlled substance registrations require a one-time SUD training completion. |
| Injectable window extended | Long-acting injectable MOUD can now be administered within 45 days of receipt, up from 14 days. |
| State laws still apply | Federal changes do not override state licensing, scope of practice, or local prescribing rules. |
Why this regulatory shift matters more than most people realize
The X-waiver was always a strange piece of policy. No other Schedule III controlled substance required a separate federal authorization to prescribe. Buprenorphine was treated as uniquely dangerous in a regulatory sense, even though its partial agonist profile actually makes it safer than many alternatives. That stigma was baked into the law, and it cost lives.
What I find most significant about the 2026 final rule is not just what it removes. It is what it signals. Treating OUD is now, officially, ordinary medicine. A primary care doctor can prescribe buprenorphine the same way they prescribe blood pressure medication. That normalization matters enormously for reducing the shame that keeps people from seeking help.
The remaining barriers are real but solvable. The one-time 8-hour training is a reasonable ask, and the cumulative completion option makes it accessible for busy clinicians. State laws will continue to vary, and some providers will be slow to adopt buprenorphine prescribing regardless of federal permission. But the structural obstacle is gone. What happens next depends on whether clinicians, health systems, and patients embrace what the law now makes possible. At Mdmatt, the belief is that every person with OUD deserves a provider who sees their condition as treatable, not shameful. This rule change makes that vision easier to act on.
— Cory
Buprenorphine treatment at Mdmatt
Mdmatt provides compassionate, patient-centered care for opioid use disorder, including Suboxone treatment and telehealth services designed to meet you where you are.
Whether you are a patient ready to start treatment or a provider looking to understand your options, Mdmatt’s team of addiction medicine specialists is here to help. The practice offers Suboxone clinic services and telehealth treatment for patients across Maryland, with locations in Owings Mills, College Park, and Nottingham. Mdmatt treats the whole person, not just the diagnosis, because lasting recovery requires addressing the root causes of addiction alongside the medical ones.
FAQ
What was the DEA X-waiver for buprenorphine?
The X-waiver was a special federal authorization, created under DATA 2000, that clinicians had to obtain before prescribing buprenorphine for opioid use disorder. It required separate training and DEA registration beyond a standard controlled substance license.
Is the DEA waiver still required in 2026?
No. The DEA formally ended the X-waiver requirement on june 8, 2026. Clinicians with a standard DEA Schedule III registration can now prescribe buprenorphine for OUD without any additional federal authorization.
What training do prescribers need now?
Clinicians applying for new or renewing DEA registrations for controlled substances must complete a one-time 8-hour training on substance use disorder treatment. This training can be completed in segments over time.
Can buprenorphine be prescribed via telehealth?
Yes. SAMHSA’s guidelines permit buprenorphine prescribing through telehealth platforms, including audio-only services, making treatment more accessible for patients in rural or underserved communities. Learn more about telemedicine Suboxone treatment and how it works in practice.
Are there still limits on how many patients a provider can treat?
Federal patient caps have been eliminated. Providers now rely on clinical judgment and must comply with any applicable state regulations when determining how many patients they treat with buprenorphine.